Mutations in tetratricopeptide repeat domain 7A (TTC7A) are associated with combined immunodeficiency with dendriform lung ossification but no intestinal atresia
Abstract
Introduction: Genetic aberrations associated with combined immunodeficiency have been increasingly identified in the past two decades. Yet, there are still 30% of these patients with unidentified genetic cause.
Methods: We employed whole genome sequencing to identify the genetic defect leading to combined immunodeficiency. Thymus, gut, and lung tissues were studied using hematoxylin and eosin staining as well as immunohistochemistry.
Results: We identified 2 deleterious mutations in the TTC7A gene. Surprisingly, the patient did not have intestinal atresia but suffered repeated infections as well fatal pneumonitis. Dendriform lung ossification developed, which was unique to this case. The patient had typical presentation of combined immunodeficiency including profound lymphopenia, markedly reduced in-vitro response to mitogens, as well as low TRECS. Serum immunoglobulins were also markedly reduced.
Conclusion: Mutations in the TTC7A gene can cause combined immunodeficiency with no intestinal atresia and predispose to lung ossification.
Statement of novelty: TTC7A mutations can cause profound immunodeficiency without multiple intestinal atresia. We report here for the first time that this defect is associated with dendriform lung ossification.
Introduction
Combined immunodeficiency (CID) defines a group of patients with profound T-cell deficiency who, unlike patients with typical severe combined immunodeficiency (SCID), have circulating T cells with various levels of dysfunction (Roifman et al. 2012). Over the past two decades the genetic aberrations underlining CID have been increasingly identified, including Zap-70 deficiency, CD25 deficiency, and others (Arpaia et al. 1994; Sharfe et al. 1997; Roifman et al. 2000). Still, in 20%–30% of patients with CID the molecular basis of their disease remains poorly defined.
One type of combined immunodeficiency was found to be associated with multiple intestinal atresias (MIA) (OMIM 2431500). This condition is usually severe and affects multiple sections of the small and large bowel (Mishalany and Der Kaloustian 1971; Guttman et al. 1973; Arnal-Monrea et al. 1983; Moreno et al. 1990; Walker et al. 1993; Gungor et al. 1995; Rothenberg et al. 1995; Moore et al. 1996; Gahukamble et al. 2002; Gahukamble and Gahukamble 2002; Bilodeau et al. 2004; Cole et al. 2010). In spite of attempts to surgically correct these lesions, outcome generally has been poor and the condition remains fatal in most affected individuals. The pathogenesis of the intestinal lesions remains unclear, although autoimmune mechanisms have been proposed, mainly because of the associated T-cell dysfunction. Most cases of MIA have been sporadic but some familial cohorts have been reported (Mishalany and Der Kaloustian 1971; Guttman et al. 1973; Arnal-Monrea et al. 1983; Moreno et al. 1990; Walker et al. 1993; Gungor et al. 1995; Rothenberg et al. 1995; Moore et al. 1996; Gahukamble et al. 2002; Gahukamble and Gahukamble 2002; Bilodeau et al. 2004; Cole et al. 2010).
Recently, genetic aberrations in the tetraticopeptide repeat domain 7A (TTC7A) gene were identified in MIA patients by using whole exome sequencing (Chen et al. 2013; Samuels et al. 2013; Bigorgne et al. 2014). However, the function of TTC7A remains poorly understood.
Multiple tetratricopeptide repeat (TPR) domains in this protein have been recognized as protein–protein interaction domains potentially involved in cellular processes such as phosphate turnover, cell cycle, and subcellular localization.
Spontaneous mutations in the mouse TTC7A ortholog Ttc7 lead to distinct phenotypes with severe skin manifestations as well as hematopoietic features, but unlike humans there is little involvement of the gut or the immune system (Beamer et al. 1995; Abernethy et al. 2000; White et al. 2004; Helms et al. 2005; Takabayashi and Katoh 2005; White et al. 2005; Takabayaski et al. 2007).
We report here for the first time a case of CID with unique features. By using whole genome sequencing on this patients DNA, 2 mutations in TTC7A were identified. Like other cases of CID this patient had chronic diarrhea, but uniquely the patient suffered dendriform pulmonary ossification and had no evidence of intestinal atresias.
Methods
Immunoglobulin and specific antibody
Serum concentrations of immunoglobulins were measured using nephelometry. Serum IgE concentration was measured using radioimmunoassay with the IgE PRIST kit (Pharmacia Diagnostics, Que.). Levels of serum antibodies to tetanus were measured using enzyme-linked immunosorbent assay, and polio antibody titres were determined using complement fixation.
T and B cell proliferative responses
Lymphocyte proliferative responses to mitogens, including phytohemagglutinin (PHA) and anti-CD3 antibodies, and to a panel of recall antigens (including candida, tetanus, herpes zoster, and cytomegalovirus) were determined using thymidine incorporation at day 3 or day 6. All assays were performed in triplicate and were compared with simultaneously stimulated randomized normal controls.
Whole genome sequencing
The whole genome of the subject was sequenced using the Complete Genomics platform. The concentration of genomic DNA sample was measured using PicoGreen in triplicate and about 11 µg of DNA was submitted to Complete Genomics for whole genome sequencing. Complete Genomics employs high-density DNA nanoarrays that are concatamers of mate pair reads, each approximately 500 bp long. Base identification is performed using a nonsequential, unchained read technology known as combinatorial probe-anchor ligation (cPAL). Each mate pair includes 35 nucleotides (nt) of genomic DNA sequence as well as adaptor sequences required for cPAL sequencing; the average mate gap length is 300 bp.
Small variants (SNV, insertions, deletions, block substitutions) as well as copy number variants were called as part of computer-generated imagery (CGI) sequencing service, using the CGI pipeline version 2.2.
Small variant quality filters
Variants were primarily quality filtered according to CGI's default quality filters, based on the variant allele fraction quality score. More stringent quality filters were defined by (i) requiring the number of supporting reads (totalReadCount) to be ≥5; (ii) requiring the estimated ploidy to be 2 for autosomes as well as for the X chromosome (the sample being female and thus having two copies of the X chromosome); (iii) requiring the equal allele fraction quality score also to be passed (score ≥40 for heterozygous, score ≥20 for homozygous calls), which penalizes variants deviating from a diploid model; (iv) requiring the ratio between reads supporting the alternate and the reference to be ≥0.35 for heterozygous variants and ≥0.80 for homozygous variants. All variants were considered, but variants passing the higher quality filters were given priority.
Small variant re-annotation pipeline
Annovar (Wang et al. 2010) and custom scripts were used to re-annotate variants (data processed in January 2014).
Variants were mapped to gene coding exons using Annovar and the RefSeq database (based on the hg19 assembly). In the presence of overlapping genomic regions (e.g., 3′ untranslated region [3′ UTR] of gene A overlapping with coding exon of gene B), Annovar follows predefined annotation precedence (e.g., coding exon has precedence over 3′ UTR).
Annovar was used to classify variants as synonymous, missense, stop-loss, stop-gain, splicing (defined as overlapping the 2 intronic bp preceding the intron–exon junction), frameshift insertion/deletions/substitutions, and nonframeshift insertion/deletions/substitutions. Alternate allele frequencies were added by Annovar using the 1000 Genome database (version: phase 1 release version 3, called from Nov. 11, 2010, alignment), National Heart Lung and Blood Institute–Exome Sequencing Project (NHLBI–ESP) (version: esp6500si) and the Complete Genomics diversity panel; for 1000 Genome and NHLBI-ESP, allele frequencies were imported for the global dataset as well as specific ethnic subgroups. Annovar was also used to map variants to dbSNP137and ClinVar entries. In particular, dbSNP was mapped matching genomic coordinates and allele and was also based only on coordinate overlap; the common polymorphism subset of dbSNP entries was additionally mapped as separate annotation fields to help remove common variants. SIFT, PolyPhen2 (HVAR version), and Mutation Assessor scores, which predicted the impact of missense variants on protein sequence, were imported from the LJB database (version 2) using Annovar. PhyloP nucleotide-level conservation scores derived from placental mammal and 100 vertebrate genome sequence alignments were imported from the corresponding UCSC tracks using custom scripts. Finally, gene–phenotype associations based on human disorders or mouse knockout or other transgenic experiments were imported using custom scripts (data downloaded and processed in August 2013).
Small variant prioritization
Variant frequency tiers were defined by requiring variants to have alternate alleles below given frequency thresholds (5%, 1%) in all the allele frequency databases used. Variants were predicted to be damaging based on the following rules: (a) all stop-gain, splicing, and frameshift; (b) missense variants with placental mammal Phylop ≥1 (or 100-vertebrate PhyloP ≥1.5) and at least one of the following five criteria satisfied: (i) SIFT score <0.05, (ii) PolyPhen2 HVAR score ≥0.95, (iii) mutation assessor score ≥2, (iv) placental mammal PhyloP score ≥2.40, and (v) 100-vertebrate PhyloP score ≥4; (c) nonframeshift insertions/deletions/substitutions with placental mammal Phylop ≥1.5 (or 100-vertebrate PhyloP ≥2.5) and not mapped to dbSNP common by exact matching or coordinate overlap. High quality, 5% rare variants matching ClinVar entries with pathogenic significance were extracted and assessed inspecting frequency and associated disorder.
All high quality, 1% rare, coding and predicted damaging variants were assigned to the following groups for more detailed investigation: (i) all homozygous, recessive mode of inheritance; (ii) potential compound heterozygous (i.e., when more than one variant satisfying the criteria above could be found per gene), recessive mode of inheritance; and (iii) all heterozygous, dominant mode of inheritance, potentially de-novo. X-linked transmission from the mother to the male affected offspring was not possible given the proband's female gender. Variants were additionally tiered based on the gene–phenotype associations: 2683 genes were found implicated in immune phenotypes in human or mouse, of which 436 had a dominant mode of inheritance in humans.
CNV annotation pipeline
Copy number gains and losses reported in “snvSegmentsDipliodBeta” were separately annotated for frequency, based on 50% reciprocal overlap with CNV called in 54 unrelated samples from the Complete Genomic diversity panel (pipeline version 2.2).
Pathology
The infant patient underwent thymus, gastric, duodenal, transverse colon, descending colon, and rectal biopsies for the investigation of immunodeficiency and diarrhea. After the patient's death, parental consent was granted to perform an autopsy limited to the chest and abdomen. The histopathology in the thymus and the patient's age matched normal thymus control; the gastrointestinal tract and lungs were also analyzed. All histochemical and immunohistochemistry stains were performed on formalin-fixed paraffin embedded tissues. Three to five µm tissue slides for microscopy were stained with hematoxlyn and eosin (H&E) after deparaffinization for light microscopy. The monoclonal antibodies used were commercially available. Antibodies against CD3, 4, 8, Mib-1, cytokeratin, and smooth muscle actin were supplied in prediluted forms by Ventana (Roche diagnostics, Tucson, AZ). For the other antibodies used, they were supplied and diluted as follows: CD133, 1/400 (AbCam, Cambridge, MA); CD163, 1/100 (Leica Bioscience Ltd., Newcastle, UK);TTF-1, 1/100 (Leica Bioscience Ltd.); Fox P3, 1/20 (Bioscience, San Diego, CA); Osteonectin, 1/50 (Biogenex, San Ramon, CA); and Cleaved Caspase3, 1/200 (Cell Signaling Technology, Danvers, MA). With the exception of cytokeratin immunostain, where protease pretreatment using enzyme and reagents from Ventana were applied, antigen retrieval procedures by heat treatment of deparaffinized tissue slides in buffered citrate solution were used. The sensitivity of the antibody binding detection was enhanced by either using Ultraview Horse Radish Peroxidase (HRP) linked multimer or a combination of biotinylated anti-antibody with Strepavidin-HRP reagents (both were from Ventana), and the antibody binding was visualized by the chromogen reaction with hydrogen peroxide and diazobenzidine. These tissue sections were counterstained with hematoxylin. Immunostains were performed with an automated immunostainer (model BenchMark XT, Ventana, Tucson, AZ).
Results
Case report
A female infant was born small for gestational age (2.46 kg) at 36 weeks to a father of Sudanese descent and a Caucasian mother. She had feeding difficulties, vomiting, diarrhea, and failure to thrive during the first four weeks of life. She suffered repeated episodes of sepsis with Staphylococcus aureus, Escherichia coli, and Serratia marcescens. At the early age of 3 months she was found to have lymphopenia. At the age of 5 months she was transferred to another hospital and again had repeated episodes of sepsis with Serratia marcescens, streptococcal pneumoniae, and Staphylococcus aureus. She was then transferred to our institution for further evaluation of her immunity. The patient developed pneumonitis due to para influenza virus and her respiratory status deteriorated gradually. In spite of maximal support treatment in the pediatric intensive care unit she died of hypoxic cardiac arrest at the age of 1 year.
Microarray analysis, karyotype, and chromosome breakage studies were normal. Genetic testing showed no abnormalities in RMRP, CD25, CD3ɛ, CD3δ, STAT1, IL-7Rα, IL-10, IL-10Rα, and IL-10Rβ.
Immune evaluation
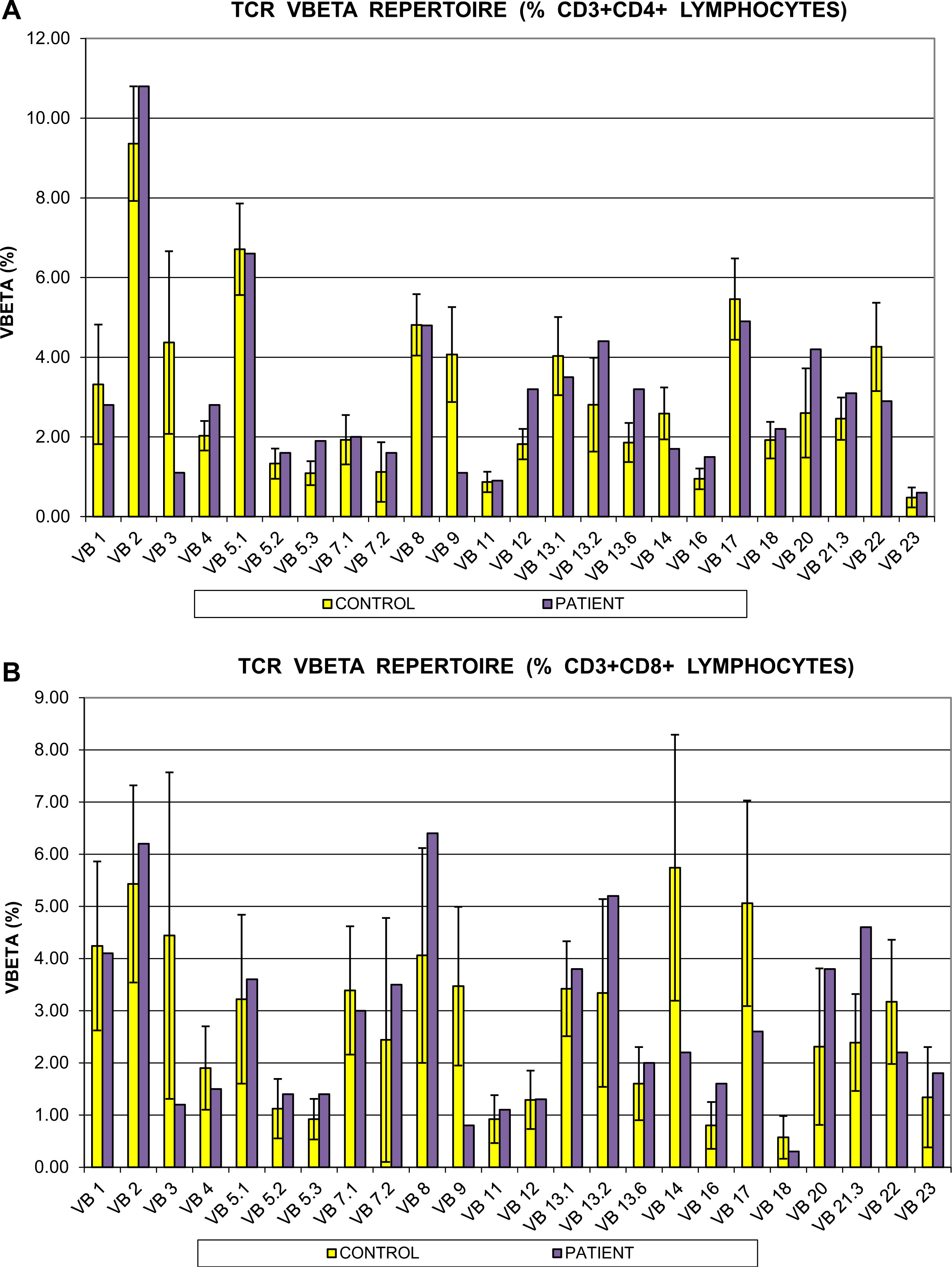
Immune evaluation revealed a low lymphocyte count with lymphocyte immunophenotyping showing CD3+ 791 cells/µL, CD4+ 365 cell/µL, CD8+ 265 cell/µL, and CD56+ 17 cell/µL cells. In vitro responses to PHA and anti-CD3 antibody stimulation were markedly reduced at <40% and <10% of controls, respectively. T-cell repertoire was also abnormal. The CD4+ cell compartment showed reduced representation of the Vβ3, Vβ9, and Vβ14 families, whereas Vβ5,3, Vβ13,2, and Vβ20 were overrepresented. Repertoire skewing was more prominent in CD8+ cells, whereby Vβ3, Vβ9, Vβ14, Vβ17, and Vβ23 families were underrepresented, with overrepresentation of Vβ21.3 only (Figure 1).
Figure 1:
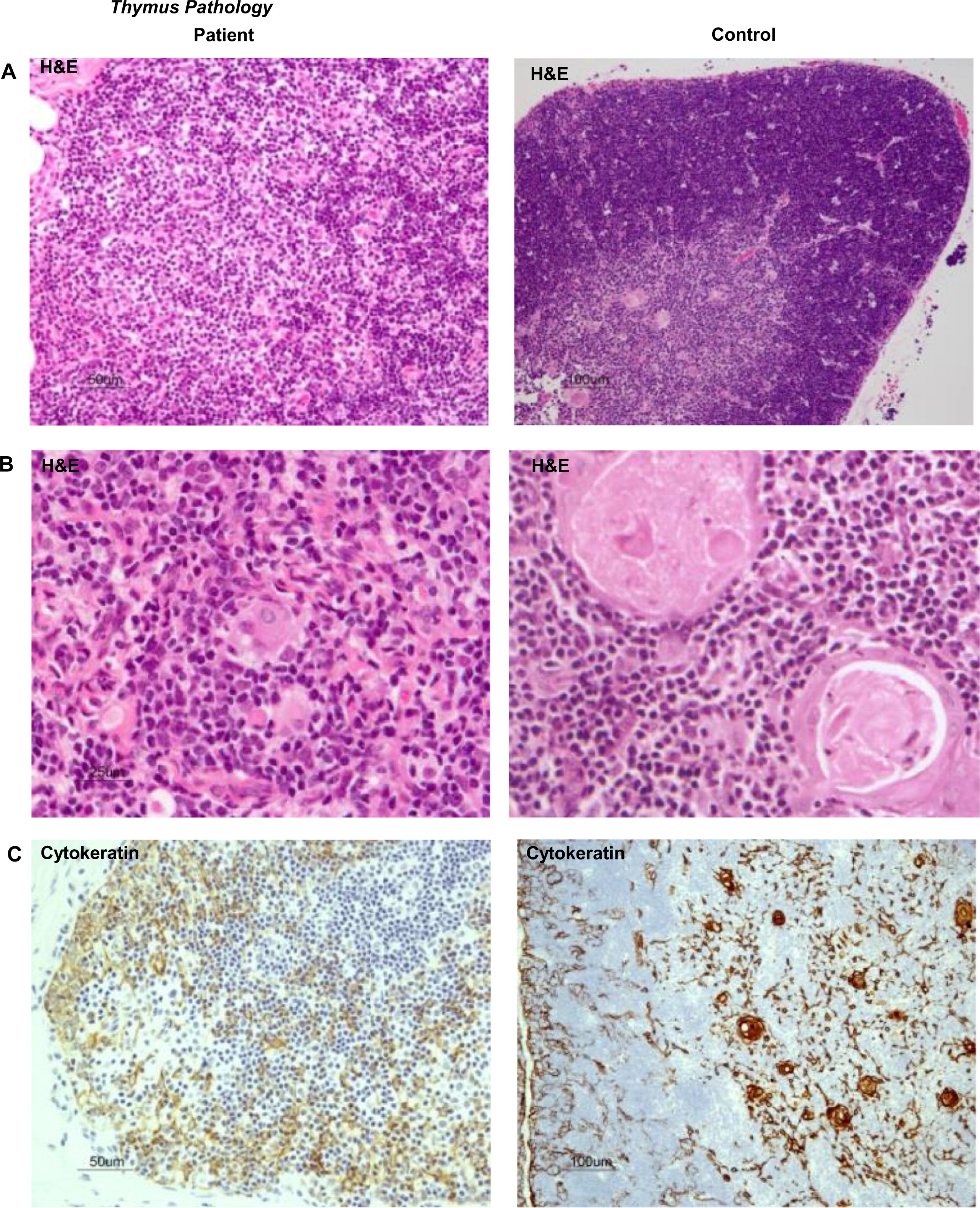
These results predicted impaired function of the thymus. We performed a thymus biopsy that showed a small and depleted gland. Most Hassall's corpuscles were small and poorly formed and their total number was markedly diminished when compared with a control (11 vs. 57 per field), thus clearly suggesting a primary immunodeficiency (Figures 2A and 2B). Corticomedullary demarcation was also compromised, with a reduced number of thymocytes in the cortical regions. Cytokeratin staining confirmed the rarity of Hassall's corpuscles and their immature nature (Figure 2C). Immunohistochemistry for CD3, CD4, and CD8 appear to show positive staining, but overall numbers were reduced in full agreement with H&E staining (Figures 2D and 2E). Remarkably, the number of FOXP3+ regulatory cells was also drastically reduced in the patient's thymus (Figure 2F). In support of the notion of a dysfunctional thymus, T-cell receptor excision circle (TREC) levels, which represent new thymus emigrants, were reduced (275 ± 120 in three different determinants).
Figure 2:
Immunoglobulins were all low (IgG < 0.6 g/L, IgA <0.2 g/L, and IgM < 0.2 g/L) and specific antibody production in response to vaccination was undetectable.
Lung pathology
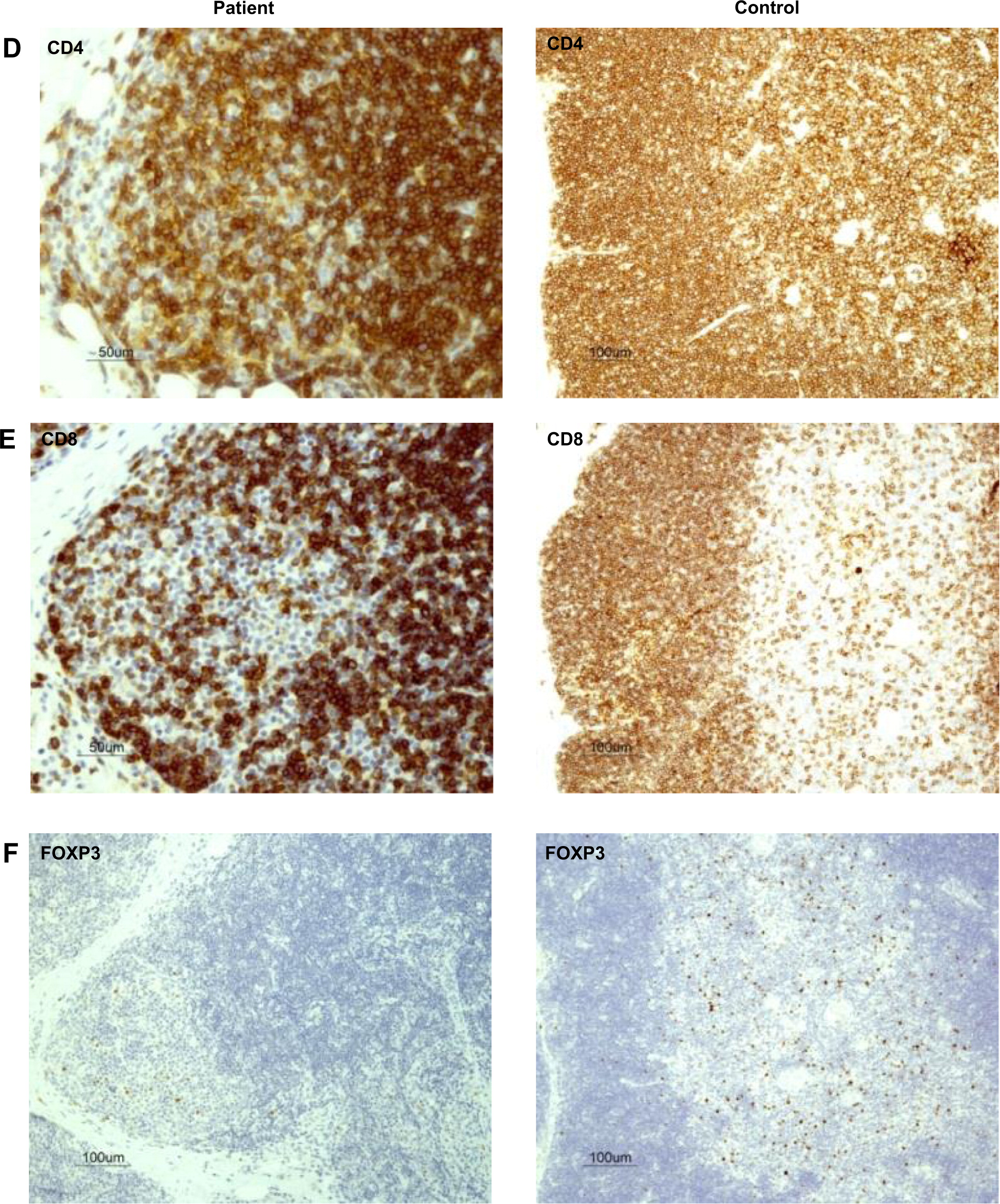
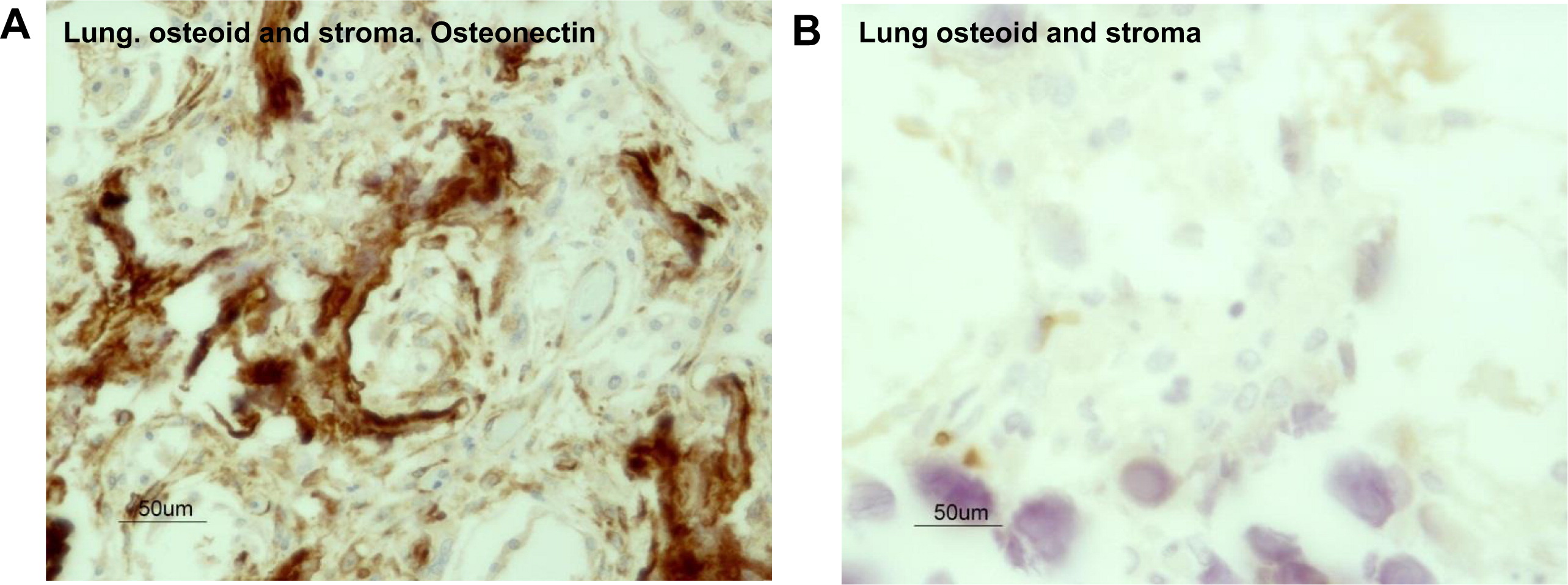
Evaluation of the autopsy lung pathology revealed diffuse alveolar damage and severe interstitial pulmonary fibrosis with honeycomb transformation of the pulmonary parenchyma (Figure 3A). There was marked reduction of alveoli and all were structurally remodeled into small round air filled microcysts that were lined with low cuboidal type-2 pneumocytes. These cells were found positive for pan cytokeratin and TTF-1 by immunostaining (Figures 3B and 3C). In addition, diffuse micro-dendriform pulmonary ossification was present. Dendriform networks of thin spicules of metaplastic osseous tissues were formed within the abnormal thick and fibrotic interalveolar septae (Figure 3A). The metaplastic osseous tissues arose within the stroma that contained smooth muscle actin expressing myofibroblasts (Figure 3D). Osteoblasts were associated with the bone spicules, and many of them showed active remodeling by osteoclasts (Figures 4A and 4B). It appeared that this osteogenic activity was in its initial stages of bone marrow development. Within the fibrotic stroma there were clear foci of hematopoeisis, such as microscopic aggregates of para-trabecular progenitor myeloid, erythroid, and megakaryocytic cells (Figures 4C and 4D). Analyses of the cell types within the microenvironment of the fibrotic interalveolar pulmonary interstium, which showed osteogenesis, demonstrated a close association between smooth muscle actin-positive myofibroblasts and macrophages that expressed the activation antigen CD163 (Figures 5A and 5B respectively). Immunostaining for the presence of osteonectin, one of the major noncollagenous proteins of bone associated with osteogenic differentiation from myofibroblasts, showed that it was expressed in the dendriform bone spicules (Figure 6A) as well as in the myofibroblasts in the vicinity of the bone spicules. Immunostaining for T cells with CD3 showed that this microenvironment was devoid of T cells (Figure 6B).
Figure 3:
Figure 4:

Figure 5:
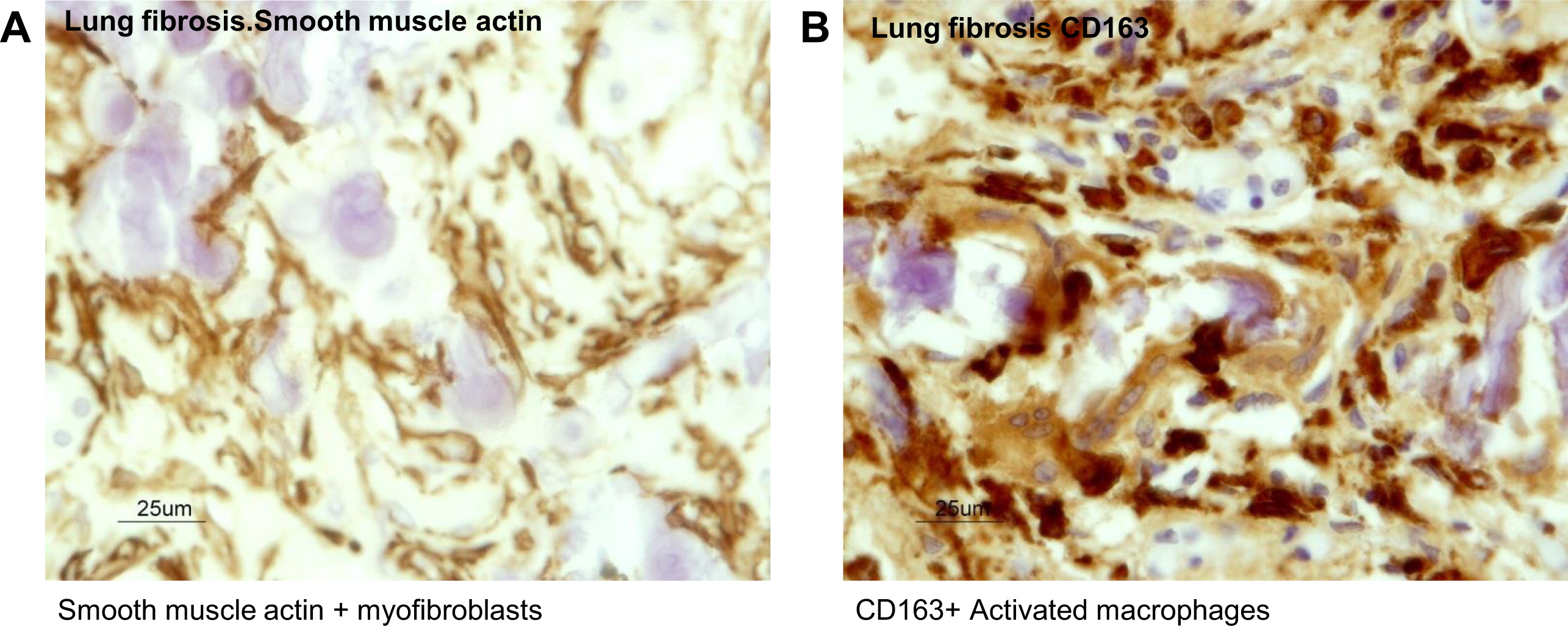
Figure 6:
There were no histological features of bronchiolitis obliterans and no residual infiltrates of chronic inflammatory cells were seen within the fibrotic pulmonary interstitium. No viral cytopathic changes were found and stains for fungi and bacteria and immunostains for adenovirus, cytomegalovirus, and respiratory syncytial virus were all negative. DNA amplification by polymerase chain reaction detected parainfluenza A (consistent with patient's history).
Gut pathology
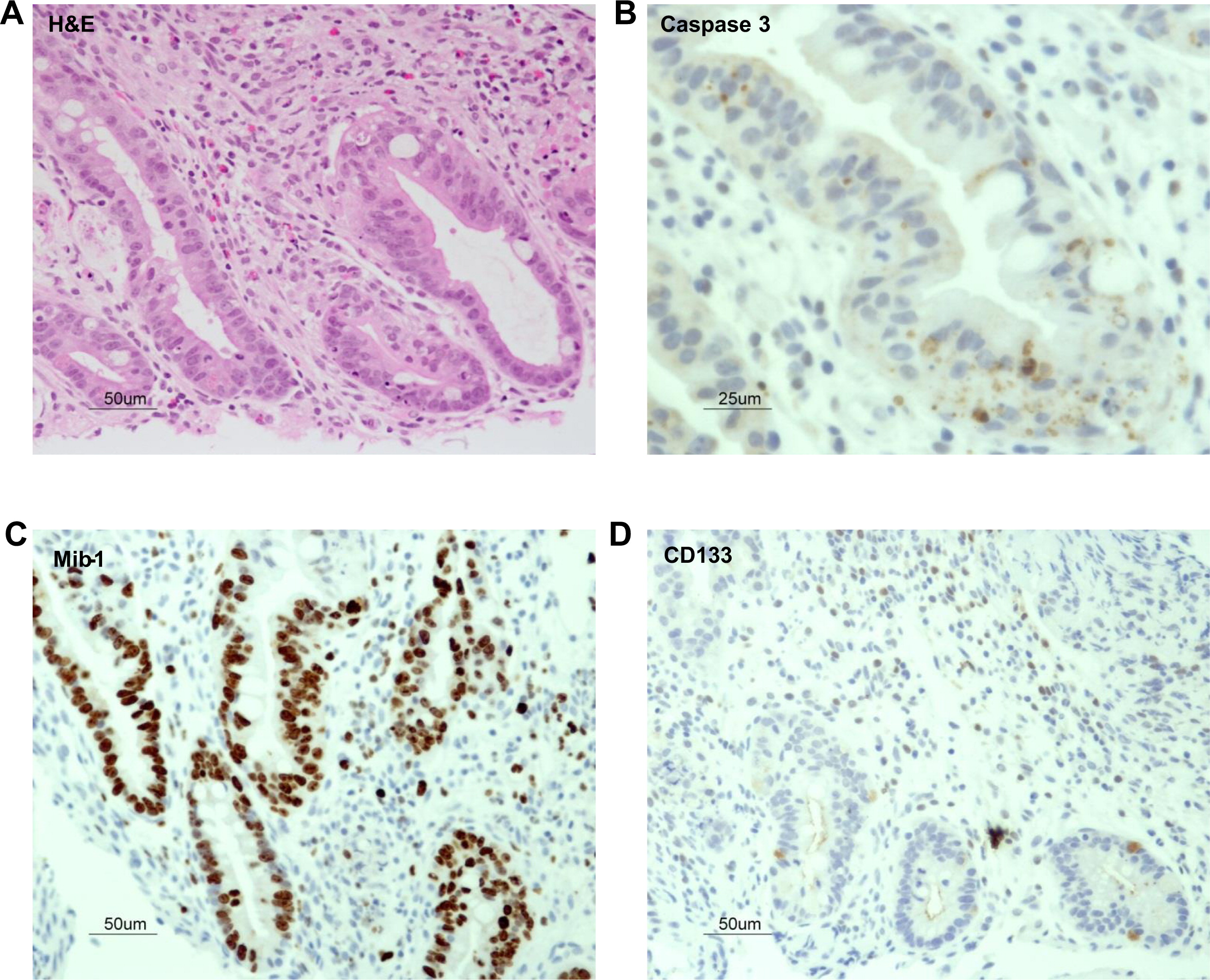
Biopsy of the duodenum showed moderate partial villous atrophy with paucity of inflammatory cells in the lamina propria. There was no evidence of tufting and there were no cytoplasmic changes consistent with microvillous inclusion disease. Periodic acid – Schiff stain demonstrated a well-preserved brush border. The colonic biopsy showed marked mucosal injury with regenerative mucosal glandular alterations. Enterocyte apoptosis was seen predominantly in the enterocytes in the basal regions of the crypts (Figure 7). Apoptosis was evidenced by expression of cleaved caspase 3 (Figures 8A and 8B) as well as structural anomalies, such as increased transit amplifying zone characterized by Mib-1 positive cells (Figure 8C) and abnormal location of CD133 positive crypt stem cells (Figure 8D). Paneth cells and neuroendocrine cells were present.
Figure 7:
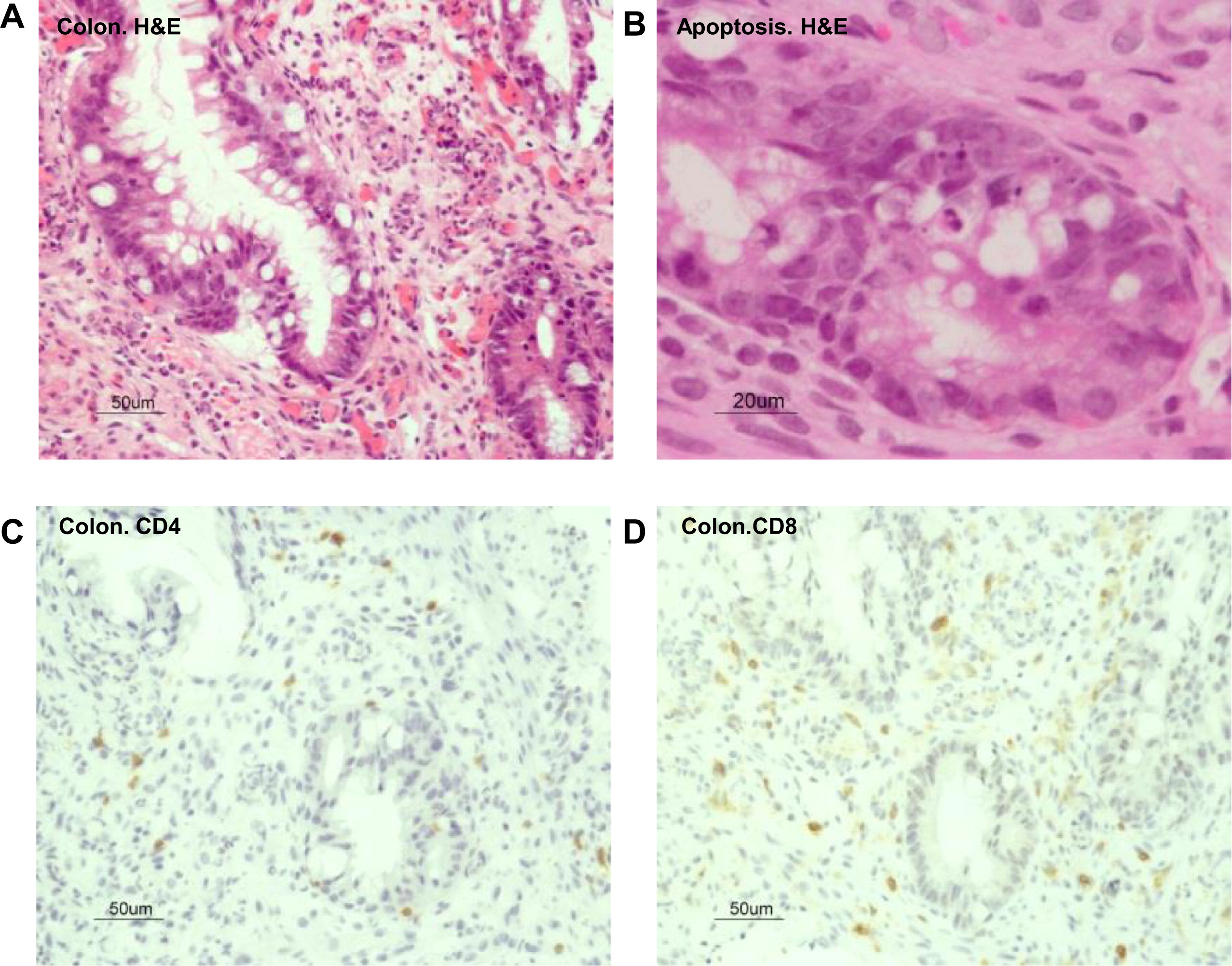
Figure 8:
Genetic analysis
To identify the underlining genetic cause of this disorder we employed whole genome sequencing. The whole genome of the patient was sequenced using the Complete Genomics Inc. (Mountain View, CA) platform.
The resulting sequencing run had >97.5% of the human genome covered by unique reads with depth 5× or greater and >95.7% with depth 10× or greater. The coding sequence coverage displayed only slightly higher percentages.
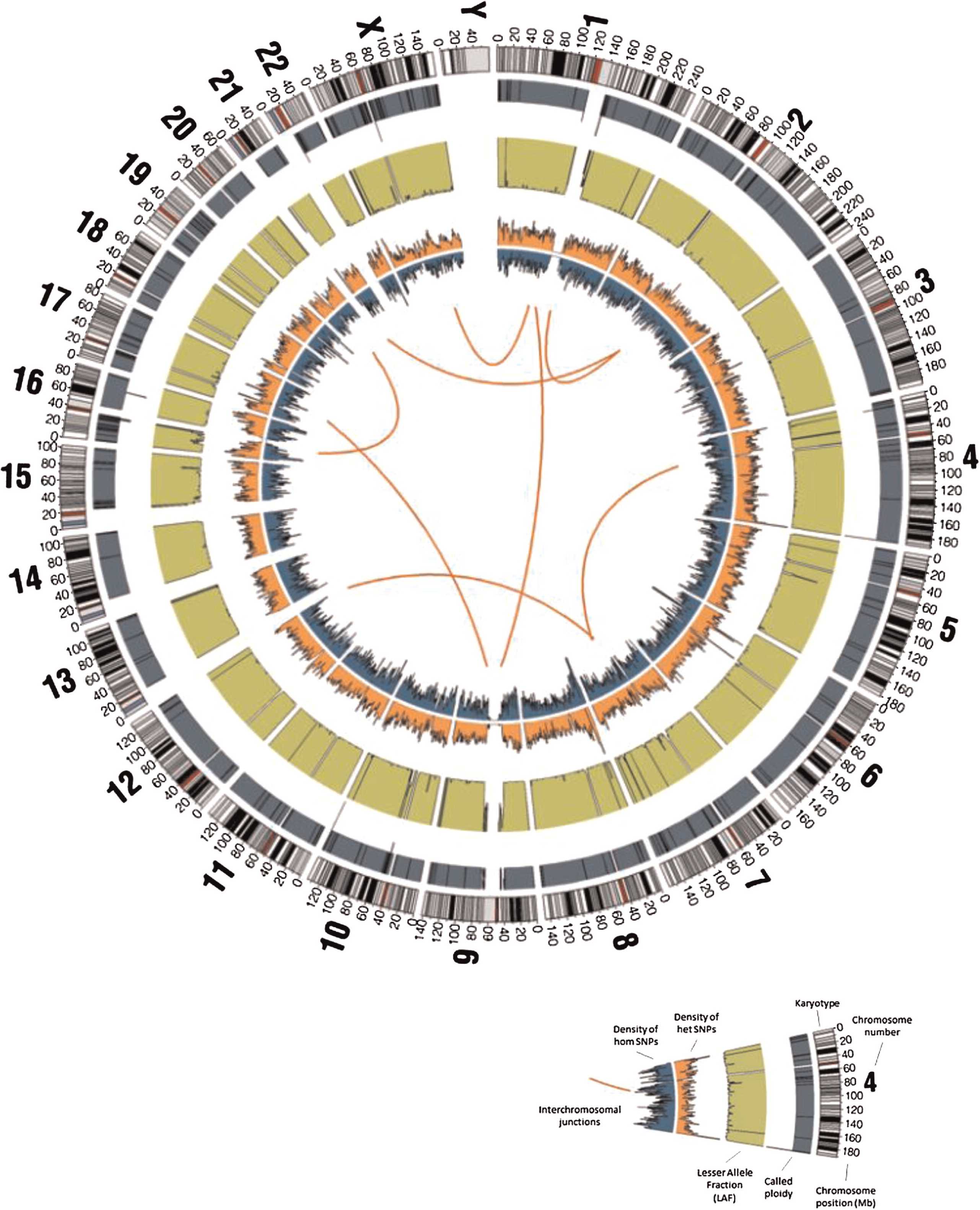
Of the 4 656 733 variants that were called (including “half calls” where only one allele is resolved), 4 161 694 (89.4%) passed CGI's default quality filters and 3 776 872 (81.1%) passed the more stringent filters. Of the variants passing quality filters, 24 512 and 22 389 (about 0.6% in both cases) were coding or splicing, respectively; of these, 2758 (11.3%) and 2240 (10%) were found to be 5% rare, of which 1595 (6.5%) and 1203 (5.4%) were found to be 1% rare (Figure 9).
Figure 9:
Three variants were of high quality, 5% rare, and matched a ClinVar pathogenic record. However, none of them matched a disorder related to the primary immunodeficiency observed in the subject (MSR1, rs72552387: Malignant tumor of prostate, SCN3B, rs121918282: Brugada syndrome 7, HAMP, rs104894696: Hemochromatosis, modifier of).
Two variants were found to be stringent high quality, coding or splicing, 1% rare homozygous, and disrupting a gene product with known immune phenotype association; both were frameshift substitutions, disrupting the genes MMP12 and ZFPM1 (chr11:102738794-102738795, MMP12:NM_002426:exon5:c.630_631AAA; chr16:88599700-88599705, ZFPM1:NM_153813:exon10:c.1334_1339CC). After close inspection, the MMP12 variant was found to be a likely reference sequence error or private variant (based on the HuRef sequence and other mammalian organisms sequence), whereas the ZPFM1 variants were in a region of dubious coding sequence accuracy.
Although it did not meet the stringent quality requirements, a potential compound heterozygous event was found for CHD4 and was prioritized for follow up because of a particularly interesting phenotype in the mouse model (abnormal T cell counts, hypoplastic thymus, abnormal spleen, liver inflammation); however, validation by Sanger sequencing failed, confirming the importance of focusing on variants with higher quality stringency.
Five variants were found to be stringent high quality, coding or splicing, 1% rare, heterozygous, and disrupting a gene product with known immune and dominant phenotype; however, none of them had clinical presentations compatible with the subject in study (TTN: hypertrophic cardiomyopathy, muscular distrophy; PLEC: epidermolysis bullosa, muscular distrophy; NUP214: acute leukemia; VWF: von Willebrand disease; ITGB3: bleeding disorder, posttransfusion purpura, Glanzmann thrombasthenia).
No rare (1%) CNV disrupted more than one gene, and none of the 6 genes with coding exons overlapped by 1% rare losses (OR5M10, FOLH1B, TRIM77, WFDC8) or 1% rare gains (ANKRD36, HYDIN) had any phenotypic or functional information implicating them in the patient's disorder.
Only one gene, TTC7A, was found to have a potential compound heterozygous event composed of two or more variants in the stringent high quality group, coding or splicing, 1% rare homozygous, and disrupting a gene product with a known immune phenotype. Interestingly, the OMIM disorder associated with TTC7A is intestinal atresia in humans. The two variants, recognized as very low-frequency damaging missense and a novel stop-gain, were inspected carefully and were confirmed to have sufficient damaging potential (TTC7A:NM_020458:exon14:c.C1576T:p.Q526X).
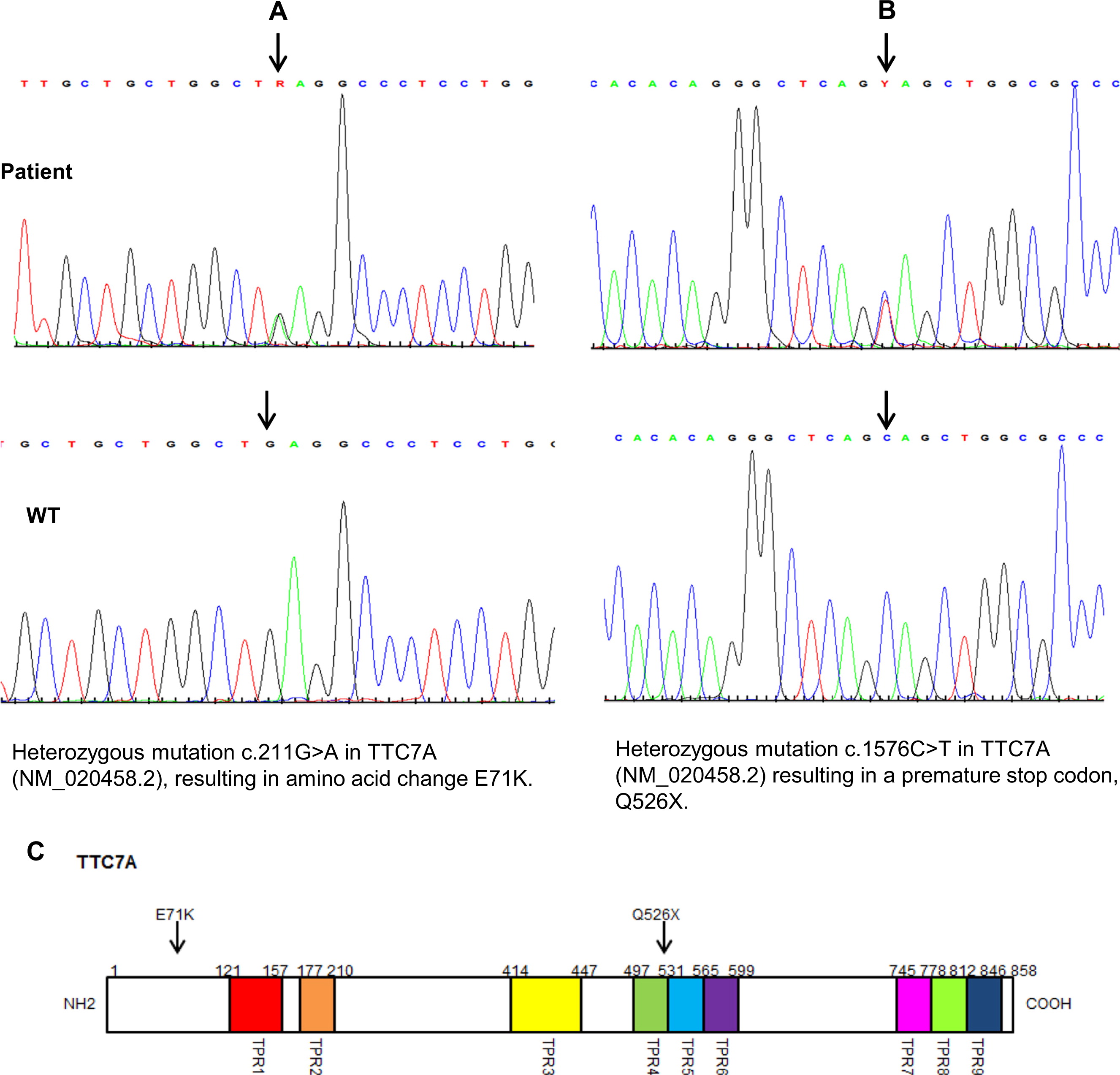
Two mutations were confirmed by Sanger sequencing in the patient's and in her parents’ TTC7A gene. The mother carried a novel heterozygous nonsense mutation in exon 14 c.1576 C > T, a substitution that results in the premature termination of the protein at amino acid 526 (p.Q526X) (Figure 10). The father was heterozygous for a G to A transition in exon 2 at position 211 (c 211 G > A), which predicts a glutamic acid to lysine substitution at position 71 (p. E71K). This mutation is likely to be deleterious (polyphen score 0.99) and located at the region predicted to be critical for protein–protein interactions (Blatck and Lassle 1992; Scheufler 2000).
Figure 10:
Discussion
MIA typically affects both the small intestine and the colon (Mishalany and Der Kaloustian 1971; Guttman et al. 1973; Arnal-Monrea et al. 1983; Moreno et al. 1990; Walker et al. 1993; Gungor et al. 1995; Rothenberg et al. 1995; Moore et al. 1996; Gahukamble et al. 2002; Gahukamble and Gahukamble 2002; Bilodeau et al. 2004; Cole et al. 2010) and is frequently fatal in spite of attempts to surgically correct the lesions (Mishalany and Der Kaloustian 1971; Guttman et al. 1973; Arnal-Monrea et al. 1983; Moreno et al. 1990; Walker et al. 1993; Gungor et al. 1995; Rothenberg et al. 1995; Moore et al. 1996; Gahukamble et al. 2002; Gahukamble and Gahukamble 2002; Bilodeau et al. 2004; Cole et al. 2010). The associated immunodeficiency is variable and the extreme cases present like T−B+ SCID or T+B+ CID (Mishalany and Der Kaloustian 1971; Guttman et al. 1973; Arnal-Monrea et al. 1983; Moreno et al. 1990; Walker et al. 1993; Gungor et al. 1995; Rothenberg et al. 1995; Moore et al. 1996; Gahukamble et al. 2002; Gahukamble and Gahukamble 2002; Bilodeau et al. 2004; Cole et al. 2010). Several groups have recently shown that MIA can be associated with mutations in the TTC7A gene (Bigorgne et al. 2014; Chen et al. 2013; Samuels et al. 2013).
Little is known about the role of TTC7A in the development or function of the immune system. Spontaneous mutations in the mouse TTC7A ortholog Ttc7 results predominantly in a skin disorder reminiscent of psoriasis as well as anemia (Beamer et al. 1995; Abernethy et al. 2000; White et al. 2004; Helms et al. 2005; Takabayashi and Katoh 2005; White et al. 2005; Takabayaski et al. 2007). The flaky skin (fsn) mouse results from an insertion of an additional exon between exons 14 and 15, thus leading to an in-frame insertion of 61 amino acids disrupting a TPR domain. This is predicted to be a protein–protein interaction domain likely interacting with components of the cell cycle process, subcellular localization, and phosphorylation events (Beamer et al. 1995; Abernethy et al. 2000; White et al. 2004; Helms et al. 2005; Takabayashi and Katoh 2005; White et al. 2005; Takabayaski et al. 2007). The immune abnormality in the fsn mouse is surprisingly mild with some reduction of CD4+ cells and lymphoid hyperplasia (Beamer et al. 1995; White et al. 2004; Helms et al. 2005; Takabayashi and Katoh 2005; White et al. 2005; Abernethy et al. 2000; Takabayaski et al. 2007).
Clearly, the phenotypes of humans and mice affected by mutations in TTC7 differ vastly. It is unclear whether such differences are species specific or if they are related to the effect of the different mutations. Future studies that elucidate the function of TTC7A will no doubt aid in better understanding this discrepancy.
The human cases described to date, had multiple intestinal atresias and various levels of immunodeficiency. The more severely immunologically affected individuals seem to have had severe combined immunodeficiency. Their thymus on autopsy was hypoplastic with reduced cellularity and partial corticomedullarly distinction (Bigorgne et al. 2014; Chen et al. 2013). Similar changes may be related to the underlying condition or possibly caused by stress or consumption of immunosuppressant drugs. However, paucity of Hassall's corpuscles as demonstrated in our case is more likely to be associated with primary immunodeficiency.
The thymus biopsy obtained from our patient showed a clear reduction in the number of Hassall's corpuscles compared with a control, but more importantly, these corpuscles were poorly and only partially formed, indicating a primary immunodeficiency. The lymphopenia, low TRECs and markedly reduced responses to mitogens and antigens were further evidence in support of this notion.
The gut involvement in MIA is interesting and has been studied in depth by several groups (Bigorgne et al. 2014; Avitzur et al. 2014). Pathological features include partial or total villous atrophy with multiple apoptotic figures (Bigorgne et al. 2014) and clear disruption of the epithelial architecture. Intestinal organoid cultures derived from the patients’ gut demonstrated inversion of apicobasal polarity of the epithelial cells, a change expected to disrupt growth and differentiation of intestinal epithelial cells (Bigorgne et al. 2014; Avitzur et al. 2014). Similar changes were observed in our patient, yet there was no sign of atresia at any segment of the gut. This may suggest the other factors may be involved in the process of developing atresia. Alternatively, it is possible that some mutations may preserve certain functions of TTC7A, thus avoiding formation of atresia.
Diffuse pulmonary ossification is an extremely rare condition. One adult case series review of autopsies performed from 1978–2004, identified only 8 cases from 1393 patients, all were 65 years and older, (Lara et al. 2005). Another review reported an incidence of 1.63 cases per 1000 autopsies (Tseung and Duflou 2006). This condition was initially noted in the literature in 1949, in patients with mitral stenosis (Lawson 1949). Since then, occurrences of this condition were reported to be associated with a variety of lung disorders with a chronic pulmonary disease, with a predilection in males (88%). Histologically, two forms can be distinguished, nodular and dendriform. The former is more commonly associated with passive pulmonary congestion that occurs with mitral valve stenosis, whereas the dendriform type appears associated with chronic lung inflammation (Tseung and Duflou 2006). There is only one report of this condition affecting a father and his son, suggesting a possible hereditary condition (Azuma et al. 2003). However, this condition was never described before in infants.
Recently, myofibroblasts have been implicated in playing an important role in the development of pulmonary fibrosis. These cells can either be derived from the bone marrow, from the resident pulmonary fibroblasts that undergo differentiation, or from the epithelial cells undergoing epithelial mesenchymal transition. Progression to fibrosis is dependent on proinflammatory and profibrotic mediators, such as transforming growth factor (TGF) β1 (Wynn 2011). Under appropriate induction conditions, fibroblasts and possibly myofibroblasts have been shown to be capable of osteogenic differentiation, evidenced by the expression osteonectin, one of the major noncollagen proteins of bone (Sommar et al. 2013). Osteonectin expression in the myofibroblasts of our patient indicated a direct role of these cells in bone formation in the lung.
In an immunocompetent host, injury to the lung triggers the secretion of interleukin (IL)-25, IL-33, and thymic stromal lymphopoietin (TSLP) from pneumocytes. These mediators can enhance Th2 differentiation and secretion of IL-4 and IL-1, cytokines that can promote secretion of TGF-β1 and other mediators from pro-fibrogenic macrophages as well as recruitment of collagen-secreting macrophages from the bone marrow. TH2 cells can also trigger an antifibrotic feedback process mediated by arginase-1 activity in M2 macrophages, which then inhibit further IL-13 production. Th-1 cells on the other hand that secrete interferon (IFN)-γ can suppress collagen synthesis in fibroblasts by activating M1 macrophages that favor degradation of extracellular matrix (ECM) (Wynn 2011). It is possible therefore that in our patient with CID, increased fibrosis may have been induced by increased profibrotic signals, lack of inhibitory signals, or both.
The intrinsic immunodefiency in this patient resulted in a high susceptibility to infections and the tissue injuries that follow pulmonary parainfluenza A infection, which could have caused injuries to the alveolar epithelium. This led to release of macrophage-stimulating cytokines that induced proliferation and recruitment fibroblasts/myofibroblasts, which resulted in the development of a fulminant course of pulmonary interstitial fibrosis and fatal respiratory failure.
We report here a unique case of combined immunodeficiency causes by mutations in TTC7A without the typical association with MIA. This is also the first description of dendriform lung ossification in an infant.
Acknowledgement
This work was supported by the Canadian Center for Primary Immunodeficiency as well as Immunodeficiency Canada. We thank Megan and Sandra for the preparation of the manuscript. This case was independently studied by other investigators (Avitzur et al. 2014); however, there is no duplication of the data. Whole genome sequencing, thymus pathology, immune work up, as well as lung pathology are all unique to this report with no overlap.
REFERENCES
Abernethy N.D., Hagan C., Tan P.L., Birchall N.M., and Watson J.D. The peripheral lymphoid compartment is disrupted in flaky skin mice Immunol. Cell Biol. 2000 78 5 -12
Arnal-Monrea F., Pombo F., and Capdevila-Puerta A. Multiple hereditary gastrointestinal atresias: study of a family Acta. Paediatrica. Scandinavica. 1983 72 773 -777
Arpaia E., Shahar M., Dadi H., Cohen A., and Roifman C.M. Defective T cell receptor signaling and CD8+ thymic selection in humans lacking Zap-70 kinase Cell. 1994 76 5 947 -958
Avitzur, Y., Guo, C., Mastropaolo, L.A., Bahrami, E., Chen, H., Zhao, Z., et al. 2014. Mutations in Tetratricopeptide Repeat Domain 7A Result in a Severe Form of Very Early Onset Inflammatory Bowel Disease. Gastroenterology, 10 January 2014. pii:.
Azuma A., Miyamoto H., and Enomoto T. Familial clustering of dendriform pulmonary ossification Sarcoidosis, Vasc. Diffuse. Lung. Dis. 2003 20 152 -154
Beamer W.G., Pelsue S.C., Shultz L.D., Sundberg J.P., and Barker J.E. The flaky skin (fsn) mutation in mice: map location and description of the anemia Blood. 1995 86 3220 -3226
Bigorgne A.E., Farin H.G., Lemoine R., Mahlaoui N., Lambert N., Gil M., et al. TTC7A mutations disrupt intestinal epithelial apicobasal polarity J. Clin. Invest. 2014 124 328 -337
Bilodeau A., Prasil P., Cloutier R., Laframboise R., Meguerditchian A.N., and Roy G. Hereditary multiple intestinal atresia: thirty years later J. Pediat. Surg. 2004 39 723 -730
Blatch G.L. and Lassle M. The tetratricopeptide repeat: a structural motif mediating protein-protein interactions Bioessays. 1992 21 11 932 -939
Chen R., Giliani S., Lanzi G., Mias G.I., Lonardi S., Dobbs K., et al. Whole-exome sequencing identifies tetratricopeptide repeat domain 7A (TTC7A) mutations for combined immunodeficiency with intestinal atresias J. Allergy. Clin. Immunol. 2013 132 2 656 -664
Cole C., Freitas A., Clifton M.S., and Durham M.M. Hereditary multiple intestinal atresias: 2 new cases and review of the literature J. Pediat. Surg. 2010 45 E21 -E24
Gahukamble D.B. and Gahukamble L.D. Multiple gastrointestinal atresias in two consecutive siblings Pediat. Surg. Int. 2002 18 175 -177
Gahukamble D.B., Adnan A.R., and Al-Gadi M. Atresias of the gastrointestinal tract in an inbred, previously unstudied population Pediat. Surg. Int. 2002 18 40 -42
Gungor N., Balci S., Tanyel F.C., and Gogus S. Familial intestinal polyatresia syndrome Clin. Genet. 1995 47 245 -247
Guttman F.M., Braun P., Garance P.H., Blanchard H., Collin P.P., and Dallaire L. Multiple atresias and a new syndrome of hereditary multiple atresias involving hastrointestinal tract from stomach to rectum J. Pediat. Surg. 1973 8 633 -640
Helms C., Pelsue S., Cao L., Lamb E., Loffredo B., Taillon-Miller P., et al. The tetratricopeptide repeat domain 7 gene is mutated in flaky skin mice: a model for psoriasis, autoimmunity and anemia Exp. Biol. Med. 2005 230 659 -667
Lara J.F., Catroppo J.F., and Kim D.U. Dendriform pulmonary ossification, a form of diffuse pulmonary ossification: report of 26 year autopsy study experience Arch. Pathol. Lab. Med. 2005 129 348 -353
Lawson H.M. Disseminated ossification of the lungs of association with mitral stenosis Br. Med. J. 1949 1 433
Mishalany H.G. and Der Kaloustian V.M. Familial multiple-level intestinal atresias: report of two siblings J. Pediat. 1971 79 124 -125
Moore S.W., de Jongh G., Bouic P., Brown R.A., and Kirsten G. Immune deficiency in familial duodenal atresia J. Pediat. Surg. 1996 31 1733 -1735
Moreno L.A., Gottrand F., Turck D., Manouvrier-Hanu S., Mazingue F., and Morisot C. Severe combined immunodeficiency syndrome associated with autosomal recessive familial multiple gastrointestinal atresias: study of a family Am. J. Med. Genet. 1990 37 143 -146
Roifman C.M., Somech R., Kavadas F., Pires L., Nahum A., Dalal I., and Grunebaum E. Defining Combined Immunodeficiency J. Allergy. Clin. Immunol. 2012 130 1 177 -183
Sharfe N., Shahar M., and Roifman C.M. An interleukin-2 receptor gamma chain mutation with normal thymus morphology J. Clin. Invest. 1997 100 12 3036 -3043
Roifman, C.M., and Dadi, H.K. 2000. Human Interleukin-2 receptor a deficiency. In Primary T cell Immunodeficiencies. Immunology, Allergy Clinics of North America. WB Saunders Company, Pennsylvania.
Rothenberg M.E., White F.V., Chilmonczyk B., and Chatila T. A syndrome involving immunodeficiency and multiple intestinal atresias Immunodeficiency. 1995 5 171 -178
Samuels M.E., Majewski J., Alirezaie N., Fernandez I., Casals F., Patey N., et al. Exome sequencing identifies mutations in the gene TTC7A in French-Canadian cases with hereditary multiple intestinal atresia J. Med. Genet. 2013 50 324 -329
Scheufler C. Structure of TPR domain-peptide complexes: critical elements in the assembly of the Hsp70-Hsp90 multichaperone machine Cell. 2000 101 2 199 -210
Sommar P., Junker J.P., and Strandenes E. Osteogenically induced human dermal fibroblasts as a tool to regenerate bone J. Plast. Surg. Hand. Surg. 2013 47 8 -13
Takabayaski S., Iwashita S., Hirashima T., and Katoh H. The novel tetratricopeptide repeat domain 7 mutation, Ttc7fsn-Jic, with deletion of the TPR-SB repeat causes severe flaky skin phenotype Exp. Biol. Med. 2007 323 695 -699
Tseung J. and Duflou J. Diffuse pulmonary ossification: an uncommon incidental autopsy finding Pathology. 2006 38 454 -458
Walker M.W., Lovell M.A., Kelly T.E., Golden W., and Saulsbury F.T. Multiple areas of intestinal atresia associated with immunodeficiency and posttransfusion graft-versus-host disease J. Pediat. 1993 123 93 -95
Takabayashi S. and Katoh H. A mutant mouse with severe anemia and skin abnormalities controlled by a new allele of the flaky skin (fsn) locus Exp. Anim. 2005 54 339 -347
Wang K., Li M., and Hakonarson H. ANNOVAR: functional annotation of genetic variants from high-throughput sequencing data Nucl. Acid. Res. 2010 38 164
White R.A., McNulty S.G., Nsumu N.N., Boydston L.A, Brewer B.P., and Shimizu K. Positional cloning of the Ttc7 gene required for normal iron homeostasis and mutated in hea and fsn anemia mice Genomics. 2005 85 330 -337
White R.A., McNulty S.G., Roman S., Garg U., Wirtz E., Kohlbrecher D., et al. Chromosomal localization, hematologic characterization, and iron metabolism of the hereditary erythroblastic anemia (hea) mutant mouse Blood. 2004 104 1511 -1518
Wynn T.A. Integrating mechanisms of pulmonary fibrosis J. Exp. Med. 2011 208 1339 -1350
Information & Authors
Information
Published In

LymphoSign Journal
Volume 01 • Number 01 • September 2014
Pages: 10 - 26
History
Received: 1 May 2014
Accepted: 6 May 2014
Accepted manuscript online: 24 June 2014
Version of record online: 24 June 2014
Authors
Metrics & Citations
Metrics
Other Metrics
Citations
Cite As
NganBo, MericoDaniele, MarcusNufar, KimVy H.D., UptonJulia, BatesAndrea, HerbrickJoanne, NalpathamkalamThomas, ThiruvahindrapuramBhooma, CoxPeter, and RoifmanChaim M.. 2014. Mutations in tetratricopeptide repeat domain 7A (TTC7A) are associated with combined immunodeficiency with dendriform lung ossification but no intestinal atresia. LymphoSign Journal.
01(01): 10-26. https://doi.org/10.14785/lpsn-2014-0002
Export Citations
If you have the appropriate software installed, you can download article citation data to the citation manager of your choice. Simply select your manager software from the list below and click Download.
Cited by
1. Gastrointestinal defects and immunodeficiency syndrome with normal in vitro IgG production
2. Whole exome and genome sequencing for Mendelian immune disorders: from molecular diagnostics to new disease variant and gene discovery
3. Abnormal apoptosis causes colitis and enteritis in patients with Hoyeraal–Hreidarsson syndrome due to DKC1 mutations
4. The effects of STAT1 dysfunction on the gut
View Options
View options
Get Access
Login options
Check if you access through your login credentials or your institution to get full access on this article.
